

RSV in babies is not just another winter cold. Respiratory Syncytial Virus is the single leading cause of infant hospitalization in the United States, responsible for up to 80,000 hospitalizations and approximately 300 deaths annually among children under five years of age. Nearly every child in America will contract RSV at least once before their second birthday, and while most recover at home with supportive care, a significant proportion develop complications that require urgent medical attention.
As a professional nanny with over ten years of hands-on experience with newborns and infants, I have witnessed firsthand how quickly RSV in babies can shift from what looks like an ordinary runny nose to a frightening breathing emergency. In this complete guide, you will find everything you need to understand RSV in babies, including how it works, how to distinguish it from a common cold, the 7 critical warning signs that require immediate medical evaluation, the safest home care strategies, and the most current 2025 prevention options now available in the United States.
What Is RSV and Why Does It Hit Babies So Hard
RSV in babies stands for Respiratory Syncytial Virus infection in infants. RSV is a highly contagious respiratory virus that infects the nose, throat, and lungs. In older children and adults, it typically causes nothing more than a mild cold lasting one to two weeks. In infants, particularly those under six months of age, the same virus can cause severe inflammation of the small airways of the lungs, a condition known as bronchiolitis, or progress to pneumonia.
The reason RSV in babies is so disproportionately dangerous compared to older children comes down to anatomy and immunity. Infants have extremely small and narrow airways. When RSV triggers inflammation and mucus buildup in those tiny passages, the obstruction has a far greater proportional impact on airflow than it would in an older child or adult. At the same time, newborns and young infants have not yet developed a mature immune response and have only the antibodies passed from their mother during pregnancy, which wane over the first months of life.
Approximately 58,000 to 80,000 children under five are hospitalized due to RSV infection each year in the US, and approximately 20 to 30 percent of infected children develop a lower respiratory tract infection such as bronchiolitis or pneumonia.
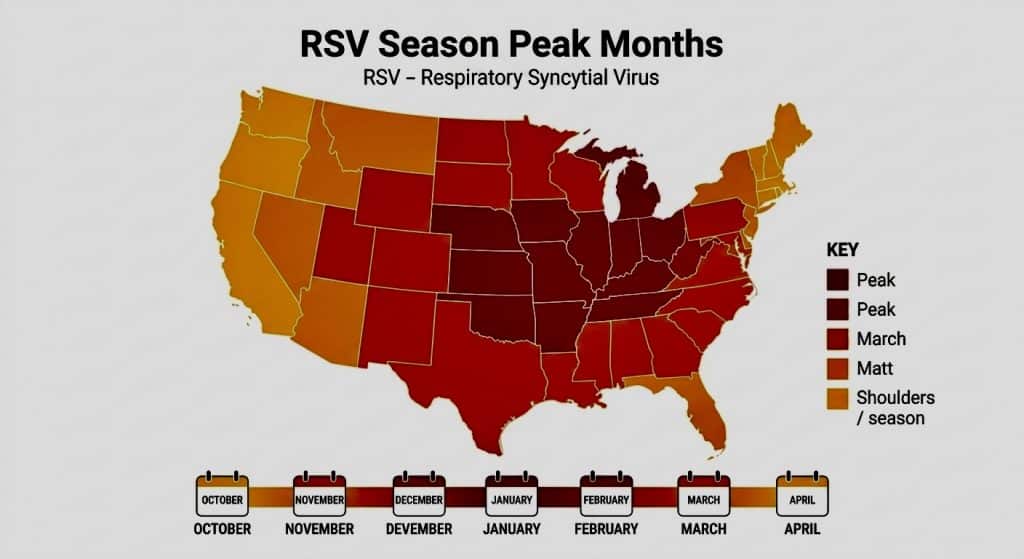
RSV spreads through respiratory droplets produced when an infected person coughs or sneezes, and through contact with contaminated surfaces. The virus can survive on hard surfaces such as tables, toys, and doorknobs for several hours, making hand hygiene and surface cleaning especially important during RSV season. In the continental United States, RSV typically circulates from the fall, peaks in December or January, and continues through the spring.
RSV in Babies vs. Common Cold: How to Tell the Difference
One of the most important skills parents can develop is recognizing when RSV in babies is moving beyond ordinary cold territory. The first two to three days of RSV often look indistinguishable from a standard upper respiratory infection. What changes, and changes rapidly in vulnerable infants, is what happens next.
Onset pattern. A common cold in a baby tends to remain stable or gradually improve after the first three to four days. RSV in babies, particularly in infants under six months, tends to worsen between days three and five, which is the window when most serious complications develop. If your baby’s symptoms are getting worse rather than better on day three or four, RSV is a strong possibility regardless of what earlier test results showed.
Breathing changes. An ordinary cold does not typically affect a baby’s breathing pattern significantly. RSV in babies frequently causes noticeable changes in how the baby breathes, including faster breathing, audible wheezing, or visible effort to pull air into the lungs. These findings are absent in a standard upper respiratory infection.
Feeding refusal. Nasal congestion from any virus can reduce feeding slightly. However, RSV in babies frequently causes pronounced feeding refusal because the combination of congestion and labored breathing makes it physically difficult and exhausting to nurse or take a bottle. Significant feeding reduction lasting more than a few hours is a meaningful clinical signal.
Duration. A typical cold resolves within seven to ten days. The cough associated with RSV in babies can persist for three to four weeks even after the acute phase has passed, which often alarms parents who expect recovery to be quicker.
7 Critical Warning Signs of RSV in Babies
Understanding when RSV in babies has crossed from manageable at home to requiring urgent care is the most important clinical skill covered in this guide. The following seven warning signs are organized from earliest concern to most critical emergency.
Warning Sign 1. Breathing Rate Faster Than Normal
A resting breathing rate of more than 60 breaths per minute in an infant under two months, or more than 50 breaths per minute in a baby aged two to twelve months, is considered abnormally fast and warrants a call to your pediatrician. You can count your baby’s breaths by watching the chest rise and fall for 30 seconds and doubling the count. If your baby’s breathing seems noticeably faster than usual at rest, RSV in babies may be causing early lower airway involvement.
Warning Sign 2. Wheezing or Noisy Breathing
A high-pitched whistling sound during exhalation, known as wheezing, indicates that the lower airways are narrowing from inflammation and mucus. Wheezing is one of the hallmark signs of bronchiolitis caused by RSV in babies. Any new wheezing in an infant, regardless of how mild it sounds, should prompt a same-day call to your pediatrician.
Warning Sign 3. Chest Retractions
Retractions are visible indentations that appear between or below the ribs, above the collarbone, or at the base of the throat when a baby struggles to breathe. When you can see the outline of your baby’s ribs with each breath, the baby is working significantly harder than normal to move air. Chest retractions are a clear sign that RSV in babies has progressed and that supplemental oxygen or hospital-level supportive care may be necessary.
Warning Sign 4. Nasal Flaring
Watch your baby’s nostrils during breathing. Nostrils that flare outward with each inhalation indicate that the baby is attempting to increase airflow by widening the nasal passage. Nasal flaring accompanying other respiratory signs is a strong indicator that RSV in babies is causing significant lower airway compromise.
Warning Sign 5. Significant Feeding Refusal
As noted above, an infant with RSV who refuses more than half of normal feedings over a six to eight hour period is at real risk for dehydration on top of the respiratory illness. When RSV in babies causes both breathing difficulty and feeding refusal simultaneously, the combination creates a compounding clinical problem that pediatricians need to assess in person, not over the phone.
Warning Sign 6. Signs of Dehydration
Because RSV in babies often causes fever alongside breathing difficulty and feeding problems, dehydration can develop quickly. Watch for fewer wet diapers than usual, dry lips and mouth, and absence of tears when crying. These are the early dehydration signals covered in detail in our post on baby dehydration signs. Dehydration on top of RSV in babies significantly increases the risk of hospitalization.
Warning Sign 7. Blue or Gray Coloring Around the Lips or Fingernails
This is the most critical warning sign of all. A blue or grayish tint around the mouth, on the lips, or under the fingernails, a condition called cyanosis, means the baby’s blood oxygen level has dropped to a dangerous level. This is a medical emergency. Call 911 immediately. Do not drive to the emergency room yourself if your baby is showing cyanosis; call for emergency services so that oxygen can be administered immediately.
High-Risk Groups: Which Babies Face the Greatest Danger from RSV
While any infant can develop severe RSV, certain groups face dramatically higher risk of complications and hospitalization. Understanding whether your baby falls into a high-risk category should influence how aggressively and how quickly you respond to early RSV symptoms.
Premature infants. Babies born before 37 weeks of gestation have smaller and less developed airways and lungs, making them significantly more vulnerable to RSV complications than full-term infants. The younger the gestational age at birth, the higher the risk.
Infants under six months of age. Regardless of birth history, very young infants lack the airway size and immune capacity to tolerate even moderate RSV-related inflammation without significant compromise. Babies born early, infants under six months, and children under two with congenital heart disease or chronic lung disease face the highest risk of complications from RSV.
Babies with congenital heart disease or chronic lung disease. Infants whose cardiac or pulmonary function is already compromised have no physiological reserve to absorb the additional burden of RSV-related airway inflammation.
Immunocompromised infants. Any baby undergoing treatment that suppresses the immune system, or who has a condition causing immune deficiency, is at elevated risk for prolonged and severe RSV illness.
Babies with neuromuscular disorders. Infants with conditions that affect their ability to swallow or clear mucus secretions are at higher risk because they cannot naturally manage the increased secretions RSV produces.
If your baby belongs to any of these groups, contact your pediatrician at the very first sign of RSV symptoms, even if the symptoms seem mild. These babies can deteriorate within hours.

How to Care for RSV in Babies at Home
There is no specific antiviral medication approved for routine treatment of RSV in babies in outpatient settings. Management focuses entirely on supportive care aimed at keeping the baby comfortable, maintaining hydration, and monitoring respiratory status closely while the immune system clears the virus. The following evidence-based strategies are recommended by the AAP and pediatric specialists for home management of mild RSV in babies.
Nasal suctioning. Clear the baby’s nasal passages using a bulb syringe or nasal aspirator (such as a NoseFrida) before every feeding and before sleep. Instilling two to three drops of saline nasal spray into each nostril before suctioning loosens thick mucus and makes the process more effective. Nasal congestion is one of the primary reasons RSV in babies interferes with feeding, and keeping the nasal passages as clear as possible significantly improves the baby’s ability to nurse or take a bottle.
Frequent, smaller feedings. Rather than attempting full feeds at normal intervals, offer smaller volumes more frequently. A congested baby who cannot breathe comfortably through the nose will fatigue quickly during feeding. Short, frequent feeds reduce the work per session and reduce the risk of vomiting from swallowing excess mucus.
Maintain adequate hydration. Continue breastfeeding on demand. For formula-fed infants, maintain regular formula feeds in smaller volumes. Hydration supports mucus clearance and overall immune function. Monitor wet diaper output throughout the illness as the primary indicator of adequate hydration.
Fever management. If your baby has a fever above 100.4°F (38°C) and is older than three months, age-appropriate doses of acetaminophen may be given as directed by your pediatrician. Never give ibuprofen to babies under six months. For fever management guidelines by age, refer to our post on fever management in babies. Never give aspirin to infants or children.
Elevate the head of the sleep surface slightly. A very slight elevation of the mattress at the head end can help with drainage and ease breathing. Place a small, firm object under the mattress itself, not under the baby. Never place pillows, towels, or wedges inside the crib with the baby.
Avoid smoke exposure. Secondhand smoke exposure significantly worsens the severity of RSV in babies. Ensure no one smokes in or near your home or vehicle during and after the illness.
Do not use over-the-counter cough or cold medications. The AAP explicitly advises against using OTC cough and cold products in children under two years old. These medications are ineffective for viral lower respiratory illness and carry real risks of side effects in infants.
Do not use humidifiers with mist. Despite being widely recommended in popular parenting sources, there is no clinical evidence that cool-mist humidifiers improve outcomes in RSV in babies, and improperly cleaned humidifiers can harbor mold and bacteria. The AAP does not recommend their use for bronchiolitis.

When to Call the Doctor and When to Go to the ER
Call your pediatrician the same day if:
- Your baby has any RSV symptoms and is under three months old.
- Your baby’s breathing seems faster than usual or slightly labored.
- Your baby is producing fewer wet diapers than normal.
- Your baby has had a fever above 100.4°F (38°C) under three months, or above 102°F (38.9°C) at any age.
- Your baby is showing mild wheezing for the first time.
- Symptoms are not improving after five to seven days.
Go to the emergency room immediately or call 911 if:
- Your baby’s lips, mouth, or fingernails appear blue or gray (cyanosis).
- Your baby has chest retractions, with visible ribs or indentations with each breath.
- Your baby is breathing very rapidly, with belly breathing or obvious respiratory distress.
- Your baby has not fed at all in six or more hours.
- Your baby is limp, unresponsive, or extremely difficult to wake.
- Breathing pauses are occurring.
For guidance on recognizing when breathing symptoms require emergency care, refer to our post on baby respiratory recovery tips.
The 2025 RSV Prevention Options Every Parent Should Know About
The landscape of RSV in babies prevention has changed dramatically since 2023, and the 2025 season brought further updates that every parent should understand before the next respiratory season begins.
Nirsevimab (Beyfortus). Approved by the FDA in 2023, nirsevimab is a long-acting monoclonal antibody administered as a single injection before or during RSV season. The AAP recommends nirsevimab for infants under eight months born during or entering their first RSV season, if the pregnant parent did not receive RSVpreF vaccine during pregnancy, if vaccination status is unknown, or if the infant was born fewer than 14 days after the parent’s RSVpreF vaccination. Data from the 2024 to 2025 RSV season showed that nirsevimab was 79% effective at preventing RSV-related hospitalization in infants.
Clesrovimab (Enflonsia). FDA-approved in 2025, clesrovimab is a second long-acting monoclonal antibody option now available for infants entering their first RSV season. Unlike nirsevimab, clesrovimab uses a fixed dose for all infants regardless of weight. Both nirsevimab and clesrovimab are now first-line recommended options by the AAP for the 2025 to 2026 season, and both are included in the Vaccines for Children Program.
RSVpreF maternal vaccine (Abrysvo). Pregnant people can receive the RSVpreF vaccine between 32 and 36 weeks of gestation, ideally between September and January. Maternal RSVpreF vaccination was associated with RSV rate reductions of 45 to 52 percent in infants under three months and 28 to 43 percent in infants under eight months during the 2024 to 2025 RSV season. Antibodies developed by the vaccinated mother transfer through the placenta to protect the baby from birth through approximately the first six months of life.
What happened to palivizumab (Synagis)? Palivizumab was the only RSV prevention product available for over two decades, requiring monthly injections throughout RSV season. Palivizumab is no longer routinely recommended and was discontinued as of December 31, 2025. Nirsevimab and clesrovimab have fully replaced it as the standard of care.
Most infants will not need both maternal vaccination and infant immunization. If the mother received RSVpreF vaccine during pregnancy at least two weeks before delivery, most infants younger than eight months do not need a separate monoclonal antibody injection. Talk to your pediatrician and obstetrician to determine which approach is appropriate for your situation.
RSV immunization timing. Infant RSV antibodies should be administered from October through the end of March in most of the continental United States. Infants born during this window should receive the antibody within one week of birth, ideally during the birth hospitalization.

RSV in Babies and the Long-Term Risk of Asthma
One aspect of RSV in babies that is increasingly recognized in pediatric research is its potential connection to long-term respiratory outcomes. Children who are hospitalized for severe RSV bronchiolitis as infants have been shown in multiple studies to have a higher likelihood of developing recurrent wheezing and asthma in later childhood compared to children without severe early RSV illness.
Researchers continue to investigate whether severe early RSV infection directly alters airway development in a way that predisposes to asthma, or whether infants who develop severe RSV are those who already have an underlying airway predisposition. Either way, preventing severe RSV in babies through currently available immunization options is a compelling strategy not only for immediate protection but potentially for long-term respiratory health.
Does RSV in Babies Provide Lasting Immunity?
This is one of the most frequently asked questions from parents whose babies have already had RSV. Unfortunately, the answer is no. RSV does not generate durable immunity. Reinfection is common throughout childhood and across the lifespan. However, subsequent infections are almost always significantly milder than the first, and the most severe complications are concentrated in the first two years of life, with the highest risk period being the first six months.
Preventing the Spread of RSV in Your Household
Preventing RSV in babies from entering your home, or limiting spread within it, requires consistent application of basic but highly effective hygiene practices.
Handwashing. Wash hands with soap and water for at least 20 seconds before handling the baby, after blowing your nose, and after returning from any public setting. Alcohol-based hand sanitizer is an effective alternative when soap and water are not available.
Surface cleaning. RSV can survive on hard surfaces for several hours. Wipe down toys, doorknobs, changing table surfaces, and any object that frequently contacts hands or mouth with an appropriate household disinfectant during RSV season.
Limit exposure during peak season. Avoid taking young infants, particularly those under three months old, to crowded indoor settings such as shopping centers, daycare facilities, or gatherings during the October to March RSV season peak. The risk-benefit analysis strongly favors limiting exposure for very young infants.
Sibling management. Older siblings frequently introduce RSV in babies by bringing the virus home from school or daycare. If an older sibling develops cold-like symptoms during RSV season, implement hand hygiene protocols immediately and minimize close contact with the baby until symptoms resolve.
Breastfeeding. Breast milk provides immunoglobulins and other immune factors that offer meaningful protection against respiratory infections during the months of exclusive breastfeeding. Maintaining breastfeeding through RSV season, as covered in detail in our post on breastfeeding benefits for baby, is one of the most evidence-based protective strategies available.

1.What are the first symptoms of RSV in babies?
RSV in babies typically begins with mild cold-like symptoms appearing two to five days after exposure. These include a runny or stuffy nose, mild cough, and low-grade fever. In the first one to two days, RSV in babies is virtually indistinguishable from any other viral upper respiratory infection. The key signal to watch for is worsening rather than improvement on days three through five, when RSV in babies most commonly progresses to lower airway involvement.
2. Is RSV in babies the same as bronchiolitis?
Not exactly. RSV is the virus; bronchiolitis is the condition it most commonly causes in infants. Approximately 80% of infant bronchiolitis cases are caused by RSV, but RSV in babies can also cause other presentations, including pneumonia and upper respiratory infection without lower airway involvement. The terms are often used interchangeably in popular literature, but clinically they are distinct concepts.
3. How long does RSV last in babies?
The acute phase of RSV in babies typically peaks around days three through five and then gradually improves over the following week. However, the cough that accompanies RSV in babies can persist for three to four weeks after the acute illness has resolved. This prolonged cough is normal and does not indicate that the infection is still active. Total illness duration from onset to complete resolution of cough is commonly two to four weeks.
4. Can I take my baby with RSV to the pediatrician or will we spread it?
Call your pediatrician’s office before going in. Most offices will direct you to a specific entrance or schedule your visit at a time that minimizes contact with other vulnerable patients. RSV in babies is highly contagious, but your baby’s clinical assessment takes priority. Never avoid seeking medical care because of concern about spreading the virus. Call first and let the office guide you.
5. Can adults get RSV from babies?
Yes, but for healthy adults the illness is typically mild and resembles a cold. Adults with underlying lung or heart conditions, or older adults over 60, can develop more serious illness from RSV. If you or another household member is immunocompromised or elderly, take extra precautions during your baby’s RSV illness, including masking, handwashing, and limiting close contact where possible.
6. Should I give my baby antibiotics for RSV?
No. RSV is caused by a virus, and antibiotics are ineffective against viruses. Antibiotics will not shorten the duration of RSV in babies, will not reduce its severity, and carry real risks of side effects and contribution to antibiotic resistance. Your pediatrician may prescribe antibiotics only if a bacterial secondary infection, such as a bacterial ear infection or bacterial pneumonia, develops alongside the RSV illness.
Summary: The RSV in Babies Action Plan
RSV in babies is the most common cause of serious respiratory illness in American infants and the leading reason babies under one year are hospitalized in the United States. The 7 critical warning signs to monitor are: faster than normal breathing rate, wheezing, chest retractions, nasal flaring, significant feeding refusal, dehydration signs, and blue or gray coloring around the lips or nails.
At home, focus on nasal suctioning, frequent small feedings, hydration monitoring, and appropriate fever management. Know your baby’s risk level, and if your baby is premature, under six months, or has an underlying health condition, act at the first symptom rather than waiting to see how things develop. For the 2025 to 2026 season, discuss nirsevimab or clesrovimab with your pediatrician before RSV season begins.
The families who navigate RSV in babies most successfully are those who observe their baby consistently, know their warning signs in advance, and act early rather than late.
Sources and References
- American Academy of Pediatrics (AAP). RSV Prevention Guidelines, Policy Statement 2025. Pediatrics, November 2025.
- Centers for Disease Control and Prevention (CDC). RSV in Infants and Young Children. Updated December 2025.
- Centers for Disease Control and Prevention (CDC). RSV Immunization Guidance for Infants. Updated August 2025.
- Cleveland Clinic. RSV in Babies and Children: Symptoms, Causes and Treatment.
- Mayo Clinic. Respiratory Syncytial Virus (RSV).
- Seattle Children’s Hospital. RSV and Bronchiolitis.
- Nationwide Children’s Hospital. What Clinicians Need to Know About RSV Prevention.
