Diabetes in children is no longer a rare diagnosis reserved for adults or elderly patients. It is a growing health crisis affecting millions of families worldwide, and in many cases it begins silently, with no obvious symptoms, in children as young as toddler age. What makes this particularly alarming is that many of the dietary habits and lifestyle patterns that increase diabetes risk are established in the earliest years of childhood, long before any diagnosis is made.
Most parents associate diabetes with sugar, and specifically with white table sugar. But the reality of diabetes in children is far more complex and far more dangerous than that single ingredient suggests. The processed food industry has introduced dozens of hidden sugars under unfamiliar names into everyday family staples, from infant cereals and flavored yogurts to seemingly healthy fruit juices and whole grain breads. Many of these sugars are metabolically more harmful than ordinary table sugar, and children are consuming them daily without their parents’ awareness.
This guide covers everything parents need to know about diabetes in children in 2026, including the critical difference between Type 1 and Type 2 diabetes, the warning signs that are most frequently missed, the hidden sugars hiding in plain sight on ingredient labels, and the evidence-based prevention strategies that can protect your child’s metabolic health from the earliest months of life.
Understanding diabetes in children starts with understanding that the food choices made in the first five years of life directly shape a child’s insulin sensitivity, pancreatic function, and long-term metabolic health. The habits your family builds today are the foundation your child’s body will build on for decades. The foundation of protecting your child begins with knowing the facts about diabetes in children that many parents simply have not been taught.
Before you continue: for guidance on establishing healthy eating habits from the earliest months, see our complete guide on starting solid foods for babies, which covers the foundations of nutritional health from the very first bites.
Table of Contents

1. Type 1 vs. Type 2 Diabetes in Children: What Every Parent Needs to Understand Before Assuming It Cannot Happen to Their Child
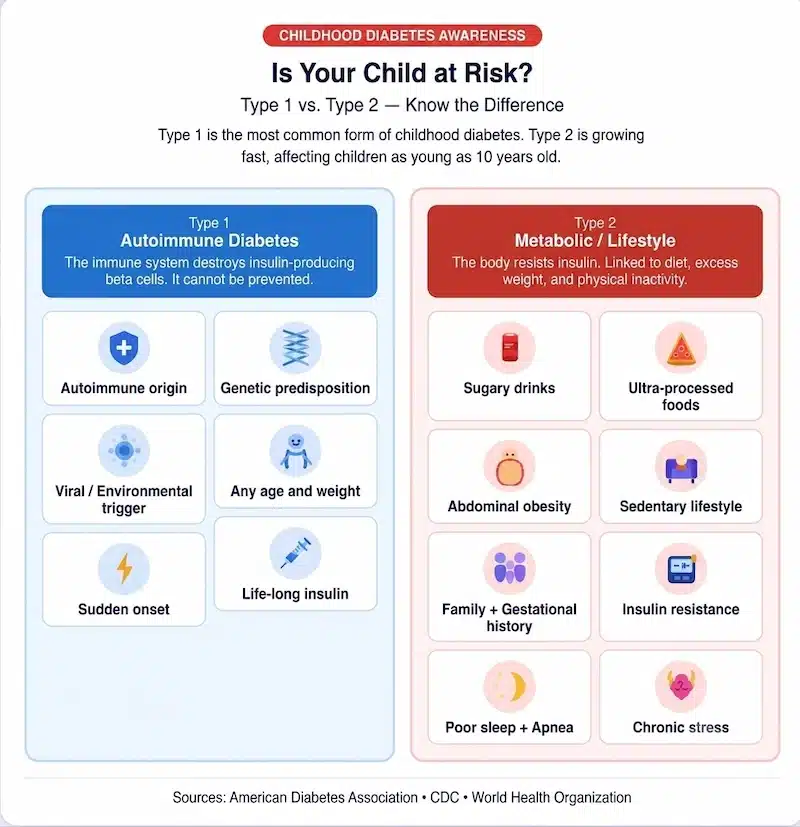
One of the most dangerous misconceptions about diabetes in children is that it is a single condition with a single cause. There are two fundamentally different forms of diabetes that affect children, and they differ in their causes, their progression, their management, and critically, their preventability.
Type 1 Diabetes in Children: The Autoimmune Form That Cannot Currently Be Prevented
Type 1 diabetes is an autoimmune condition in which the body’s immune system mistakenly attacks and destroys the insulin-producing beta cells in the pancreas. Children with Type 1 diabetes produce little to no insulin and require daily insulin administration to survive. It is not caused by diet, sugar consumption, or lifestyle choices. It can develop in any child at any age, from infancy through adolescence, and its onset is often sudden and dramatic.
The CDC confirms that Type 1 diabetes is when the body does not produce enough insulin, the hormone that balances blood sugar levels, and that there is no known way to prevent Type 1 diabetes at this time. This is a critical distinction because parents of children newly diagnosed with Type 1 diabetes often experience unnecessary guilt, wondering whether something they did or fed their child caused the condition. The current scientific consensus is clear: Type 1 diabetes is an autoimmune event, not a lifestyle consequence.
What parents can control is how quickly Type 1 diabetes is identified when symptoms appear, which determines how well its complications can be prevented. Delayed diagnosis is one of the leading causes of serious complications including diabetic ketoacidosis, a potentially life-threatening emergency that can develop within days of symptom onset.
Type 2 Diabetes in Kids: The Form That Is Growing and the One Parents Can Directly Influence
Type 2 diabetes tells a very different story. The CDC reports that type 2 diabetes is increasing in children and teens in the United States, and that insulin resistance, when the body cannot use insulin properly, is a major risk factor for type 2 diabetes for kids and adults.
Unlike Type 1, Type 2 diabetes in kids develops gradually through a process of progressive insulin resistance, a condition in which the body’s cells stop responding effectively to insulin signals. The pancreas compensates by producing more and more insulin until it can no longer keep up with demand, at which point blood sugar levels begin to rise. This process can take years, which means there is a meaningful prevention window for families who understand the risk factors and act early.
The WHO confirms that type 2 diabetes is often preventable, and that factors contributing to its development include being overweight, not getting enough exercise, and genetics, with early diagnosis being important to prevent the worst effects.
The rise of Type 2 diabetes in kids is directly linked to the rise of processed food consumption, sedentary lifestyles, and the dramatic increase in childhood obesity over the past three decades. This is not a genetic inevitability for most children. It is a dietary and lifestyle consequence that begins forming in the earliest years, and it is one that parents have more power to address than they realize.
2. The 9 Critical Warning Signs of Diabetes in Children That Parents Most Frequently Miss
The warning signs of diabetes in children are often subtle in the early stages and easy to attribute to other causes. Many parents discover their child’s diagnosis only after a routine blood test or after symptoms have been present for weeks or months without recognition. Knowing these signs can be the difference between early management and a preventable emergency.

Image credits: Photo: Pexels
Recognizing Diabetes Symptoms in Children Before They Escalate
1. Excessive thirst that seems impossible to satisfy. A child with uncontrolled blood sugar experiences osmotic thirst as the kidneys attempt to flush excess glucose through urine. A child who is drinking unusually large amounts of water and still complaining of thirst deserves a blood sugar evaluation.
2. Frequent urination, including nighttime accidents in a previously toilet-trained child. When blood sugar is elevated, the kidneys cannot reabsorb all the glucose, and it spills into the urine, pulling large amounts of water with it. Bedwetting in a child who was previously dry at night is one of the most frequently overlooked early diabetes symptoms in children.
3. Unexplained weight loss despite normal or increased appetite. In Type 1 diabetes, the body begins breaking down fat and muscle for energy because it cannot access glucose without insulin. A child who appears to be eating normally or even more than usual but is losing weight should be evaluated immediately.
4. Fatigue and lethargy that does not respond to rest. When cells cannot access glucose for energy, children feel chronically exhausted. This fatigue is often dismissed as growth spurts, poor sleep, or busy schedules, making it one of the most delayed-recognition diabetes symptoms in children.
5. Blurred vision. Elevated blood sugar causes fluid changes in the lenses of the eyes, affecting their ability to focus. A child complaining of blurry vision who has not had previous eye problems may be experiencing early diabetic changes.
6. Slow-healing cuts, scrapes, or infections. High blood sugar impairs immune function and circulation, reducing the body’s ability to repair tissue damage. Wounds that take longer than expected to heal, or infections that recur, can indicate insulin dysregulation.
7. Fruity-smelling breath. This specific symptom indicates diabetic ketoacidosis (DKA), a medical emergency in which the body begins burning fat for fuel in the absence of insulin, producing ketones as a byproduct. If your child’s breath smells fruity or like nail polish remover, seek emergency medical care immediately.
8. Darkened, velvety skin patches in body folds. A condition called acanthosis nigricans, characterized by dark, thickened skin typically appearing on the back of the neck, armpits, or groin, is a visible sign of insulin resistance in children. It is not a sign of poor hygiene. It is a metabolic signal that warrants immediate medical evaluation.
9. Irritability, mood changes, and difficulty concentrating. Blood sugar fluctuations directly affect brain function and emotional regulation. Children with undiagnosed diabetes in children frequently show behavioral changes, difficulty focusing at school, and emotional volatility that is attributed to other causes before the metabolic connection is identified.
3. The Hidden Sugar Crisis: What Is Really in Your Child’s Food and Why It Matters More Than You Think
The most dangerous aspect of the modern food environment for children is not the candy aisle. It is the breakfast cereal aisle, the flavored yogurt section, the fruit juice refrigerator, and the condiment shelf. Hidden sugars in children’s food are embedded in products marketed specifically to families as healthy, convenient, and child-friendly options.
The Sugar Names That Food Labels Use to Hide What You Are Actually Feeding Your Child
The American Heart Association notes that added sugars have a host of names on food ingredient labels, such as high fructose corn syrup, dextrose, fructose, fruit juice, and more, and that added sugar is not just present in cakes and cookies but can show up in a wide variety of foods such as Chinese chicken salad, barbecue sauce, hamburger buns, and salad dressings.
The following are the most commonly used hidden sugars in children’s food that parents must learn to identify:
High Fructose Corn Syrup (HFCS): the most researched and most concerning of all hidden sugars. HFCS has been linked to increasing triglyceride levels, which raises the risk of cardiovascular disease, and insulin resistance, which can lead to type 2 diabetes. It is found in sodas, flavored fruit drinks, ketchup, salad dressings, bread, breakfast cereals, flavored yogurts, and hundreds of other processed foods marketed to children.
Fructose in excess: when consumed beyond what whole fruits naturally provide, isolated fructose bypasses the normal satiety signals that glucose activates, meaning the brain does not register fullness. This leads to overconsumption, liver fat accumulation, and progressive insulin resistance without the child feeling that they have overeaten.
Inverted sugar and corn syrup solids: these are refined forms of sugar that the food industry uses specifically because they are absorbed more rapidly than sucrose, extending shelf life and enhancing the sweetness profile of processed products. Both cause rapid blood sugar spikes followed by compensatory insulin surges.
Agave nectar: widely marketed as a natural, healthier alternative to sugar, agave is actually composed of 70% to 90% fructose, making it metabolically one of the most harmful sweeteners available. Parents who choose agave over table sugar believing they are making a healthier choice for their children are in many cases making a more harmful one.
Dextrose, maltose, sucrose, and fruit juice concentrate: all of these are sugars that raise blood glucose and contribute to insulin resistance when consumed regularly. Their presence on an ingredient label, especially near the top of the list, indicates that the product is a significant source of added sugar regardless of what the front-of-package marketing claims.
The Products Most Likely to Contain Hidden Sugars in Children’s Food
Parents are often shocked to discover hidden sugars in children’s food in the following categories:
Flavored yogurts marketed to children can contain 12 to 28 grams of added sugar per serving, exceeding the entire daily recommended limit for a child under 10 years old in a single snack. Fruit juice, including 100% fruit juice, delivers concentrated fructose without the fiber that slows absorption in whole fruit. A single 8-ounce glass of orange juice contains the sugar of four to five whole oranges without any of their fiber.
Granola bars and breakfast cereals positioned as whole grain and high fiber frequently contain multiple added sugars that together exceed 15 grams per serving. Flavored instant oatmeal, sports drinks marketed to young athletes, and even some infant cereals and purees contain added sugars that establish early taste preferences for sweetness that drive overconsumption throughout childhood.
Children’s Hospital of Orange County reports that consuming large amounts of added sugars puts children at higher risk for obesity, high blood pressure, high cholesterol, cardiovascular disease, fatty liver disease, diabetes, and dental cavities.
4. How Insulin Resistance in Children Begins Long Before Any Diagnosis Is Made
Insulin resistance in children is not a sudden event. It is a gradual process that unfolds over months and years of metabolic stress, and it typically begins far earlier than parents expect. Understanding this timeline is essential for parents who want to intervene before the process progresses to prediabetes or full Type 2 diabetes.

Image credits: Photo: Pexels
The Step-by-Step Progression from Normal Metabolism to Type 2 Diabetes in Kids
The progression begins with repeated blood sugar spikes. Every time a child consumes a high-sugar food or beverage, blood glucose rises rapidly, triggering the pancreas to release a surge of insulin to bring it back down. In a healthy metabolic state, this process is efficient and the blood sugar returns to normal quickly.
When these spikes occur repeatedly throughout the day, as they do in children whose diets are high in processed foods, sweetened beverages, and refined carbohydrates, the body’s cells begin to develop resistance to insulin signals. The cells, overwhelmed by the constant presence of high insulin, essentially downregulate their receptors. This is insulin resistance in children in its earliest stages, and it produces no obvious symptoms.
The pancreas responds to this resistance by producing even more insulin to achieve the same effect. Over time, this overworked response becomes less efficient, and blood sugar levels begin remaining elevated for longer after meals. This stage is called prediabetes, and research consistently shows that it is present in a significant proportion of overweight children, many of whom are never screened.
Eventually, if the metabolic stress continues without intervention, the pancreatic beta cells become exhausted from years of overproduction and begin to fail. At this point, blood sugar can no longer be controlled adequately, and a formal diagnosis of Type 2 diabetes follows. This entire progression from healthy metabolism to diagnosis can take anywhere from five to fifteen years, which is why the dietary habits established in the earliest years of childhood carry such profound long-term consequences.
5. The Long-Term Dangers of Uncontrolled Diabetes in Children That Parents Must Not Underestimate
The urgency of understanding and preventing diabetes in children is not simply about managing blood sugar numbers. It is about protecting organ systems that, once damaged, cannot be fully repaired. The complications of uncontrolled diabetes are among the most severe and quality-of-life-altering conditions in medicine, and they are entirely preventable with early intervention.
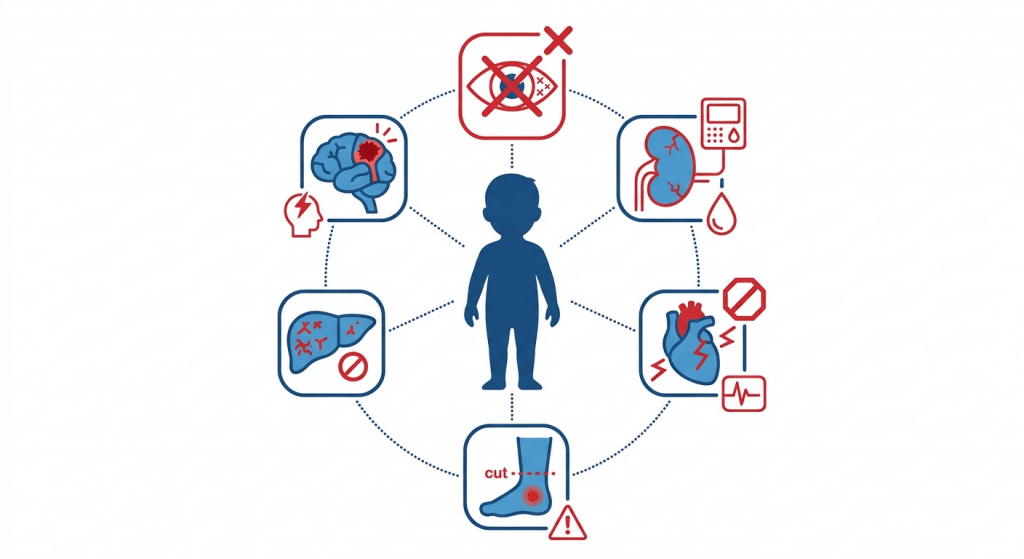
How Diabetes Damages the Body Over Time When Left Unmanaged
Vision loss and blindness. Diabetic retinopathy, damage to the blood vessels in the retina, is the leading cause of blindness in working-age adults. In children with diabetes in children that is poorly controlled over years, retinal damage can begin during adolescence, with blindness becoming a risk by early adulthood. The damage is irreversible once it progresses past certain stages, which is why blood sugar control from the time of diagnosis is critical to preserving vision for life.
Kidney disease and kidney failure. Diabetic nephropathy, progressive damage to the kidney’s filtering structures, is the leading cause of kidney failure in the United States. Children who develop diabetes in childhood and manage it poorly for decades face a significantly elevated risk of requiring dialysis or kidney transplantation in their adult years.
Cardiovascular disease. Chronically elevated blood sugar damages the walls of blood vessels throughout the body, accelerating atherosclerosis, the buildup of plaques that narrows arteries. Children with diabetes in children carry a significantly elevated lifetime risk of heart attack and stroke compared to their peers, with cardiovascular events often occurring decades earlier than in the general population.
Neuropathy and limb amputation. Diabetic neuropathy, nerve damage caused by prolonged exposure to high blood sugar, typically begins in the feet and lower legs. It produces burning, tingling, or numbness, and eventually eliminates sensation entirely. The absence of sensation means that injuries go unnoticed and infections progress to the point where amputation becomes medically necessary. Diabetes is the leading non-traumatic cause of lower limb amputation in the United States.
Liver disease. Non-alcoholic fatty liver disease (NAFLD) is directly linked to insulin resistance and excess fructose consumption. In children with high-sugar diets and progressing insulin resistance, fatty liver disease can develop years before any diabetes diagnosis and can progress to cirrhosis in adulthood if not addressed.
Cognitive and neurological effects. Emerging research links chronically elevated blood sugar and insulin resistance to impaired memory, reduced learning capacity, and increased risk of neurodegenerative conditions including Alzheimer’s disease, impaired memory, reduced learning capacity, and increased risk of neurodegenerative conditions.
6. Childhood Diabetes Prevention: What the Research Actually Tells Parents They Can Do Right Now
The research on childhood diabetes prevention is unusually encouraging for parents who engage with it. For Type 2 diabetes in particular, the evidence is strong and consistent: lifestyle interventions in children produce measurable, meaningful reductions in diabetes risk, and they work faster and more durably than any medication.

The Family-Based Prevention Strategies That Research Consistently Supports
The CDC recommends that families help kids take action to prevent type 2 diabetes while they’re young, noting that starting early can help kids develop a lifetime of healthy habits, and that healthy changes become habits more easily when everyone does them together.
Eliminate sugar-sweetened beverages entirely. This single change has more impact on childhood insulin resistance than almost any other dietary intervention. Sodas, sports drinks, flavored milks, fruit juice, and sweetened teas deliver concentrated sugar directly into the bloodstream without fiber or nutrients to slow absorption. Replacing these with water and plain milk as the household default removes one of the primary drivers of insulin resistance in children at essentially zero cost.
Prioritize whole foods over processed foods. Every whole fruit contains the sugar fructose, but it also contains fiber, water, and nutrients that slow its absorption and moderate the insulin response. The same amount of fructose in a processed juice or sweetened beverage is absorbed three to five times faster, producing a far more damaging metabolic response. Teaching children to eat the apple rather than drink the juice is a simple framing that carries significant metabolic consequences.
Establish daily physical activity as a non-negotiable family habit. Physical activity directly improves insulin sensitivity at the cellular level. Children who engage in at least 60 minutes of moderate physical activity per day show measurably better insulin sensitivity than sedentary peers, regardless of body weight. Movement does not need to be structured exercise. Active play, family walks, dancing, and outdoor activities all count.
Limit ultra-processed foods as a category. Ultra-processed foods, those containing five or more ingredients including chemical additives, flavor enhancers, and multiple added sugars, are the primary delivery vehicle for the hidden sugars discussed earlier in this guide. Shifting the household food environment away from ultra-processed options and toward minimally processed whole foods systematically reduces sugar exposure without requiring calorie counting or restrictive dieting.
Start early. Research indicates that a child should not be introduced to added sugar, especially under the age of two, and that if they never have it, they will not want it, with the principle being that influencing a child’s food choices from infancy can make a difference in their entire life.
7. How to Read a Food Label and Identify Hidden Sugars Before They Reach Your Child’s Plate
Reading food labels effectively is one of the most practical skills parents can develop for protecting their child’s metabolic health. The food industry uses more than 60 different names for added sugar on ingredient labels, but once parents understand the patterns, identifying them becomes significantly easier.

The Label-Reading System That Identifies Hidden Sugars in Children’s Food in Under 30 Seconds
Step 1: Check the serving size first. Manufacturers frequently set serving sizes smaller than what a child would actually eat in a single sitting, which makes the sugar content appear lower than it actually is. Always calculate the sugar content for the actual portion your child will consume.
Step 2: Look at Added Sugars on the Nutrition Facts panel. Since 2021, the FDA has required manufacturers to list added sugars separately from total sugars. This single line tells you how much sugar was added to the product beyond what naturally occurs in the ingredients. For children under 2, the target is zero grams of added sugar. For children 2 to 18, the American Heart Association recommends no more than 25 grams of added sugar per day total across all food and beverage sources.
Step 3: Scan the ingredient list for sugar aliases. Any ingredient ending in “-ose” is a sugar: glucose, fructose, sucrose, maltose, dextrose, galactose. Syrups of any kind are sugars: corn syrup, rice syrup, malt syrup, agave syrup, maple syrup. Juice concentrates, molasses, honey, and “natural sweeteners” are all added sugars regardless of their perceived health status.
Step 4: Check how high sugar appears in the ingredient list. Ingredients are listed in descending order by weight. If any form of sugar appears in the first three ingredients, the product is predominantly sugar by composition, regardless of what the front-of-package claims about being natural, organic, or made with real fruit.
For additional guidance on building a nutritionally sound diet for your growing child, see our complete resource on healthy eating for families.
8. Building a Diabetes-Protective Diet for Your Family Starting Today
Prevention of diabetes in children does not require perfection, nutritional expertise, or expensive specialty foods. It requires consistent application of a small number of evidence-based principles that, when maintained over months and years, fundamentally reshape a child’s metabolic trajectory.
The Daily Habits That Build Lifelong Insulin Sensitivity in Children

Make water the default beverage from infancy. Children raised on water as their primary beverage do not develop the taste expectation for sweetness that drives overconsumption of sugary drinks later in childhood. This single habit, established before 12 months of age, has lifelong metabolic implications.
Serve vegetables at every meal, even breakfast. Vegetables provide fiber that slows glucose absorption, micronutrients that support insulin function, and volume that promotes satiety without caloric excess. Children who grow up eating vegetables at every meal develop taste preferences that support healthy metabolic function throughout life.
Choose whole fruit over fruit products. Whole fruits deliver natural sugars alongside fiber, water, vitamins, and antioxidants. The fiber in a whole apple slows fructose absorption significantly compared to apple juice, apple sauce with added sugar, or apple-flavored snack products. Teaching children to default to whole fruit for sweetness rather than processed fruit products is one of the highest-impact nutritional habits parents can establish.
Limit refined carbohydrates alongside sugar. White bread, white rice, crackers, and pasta made from refined flour all convert to glucose rapidly in the body, producing blood sugar spikes that drive insulin resistance over time. Replacing refined carbohydrates with whole grain versions, sweet potatoes, legumes, and other complex carbohydrates substantially reduces the glycemic burden of each meal.
Model the habits you want your child to keep. Research consistently shows that children’s dietary preferences are shaped primarily by household food availability and parental modeling. A parent who chooses water over soda, fruit over candy, and whole grains over white bread in daily family life is providing the most powerful nutrition education available, without a single formal lesson.
For guidance on establishing these habits in the earliest months of childhood, when taste preferences are most malleable, see our complete guide on newborn care essentials.
9. When to See a Doctor About Diabetes in Children and Exactly What to Ask
Many pediatricians do not routinely screen for diabetes in children or prediabetes or insulin resistance in children unless specific risk factors are present. This means that parents who are concerned about their child’s metabolic health may need to be proactive in requesting appropriate testing.
The Specific Tests to Request and the Risk Factors That Should Prompt Screening
The CDC recommends that if a child has any two risk factors, parents should talk to their doctor about getting their child’s blood sugar tested, with testing typically beginning at 10 years old or when puberty starts, whichever is first, and repeated every 3 years.
Risk factors that warrant earlier or more frequent screening include a family history of Type 2 diabetes in a parent or sibling, overweight or obesity as defined by BMI-for-age charts, physical inactivity, signs of insulin resistance such as acanthosis nigricans, high blood pressure, or elevated cholesterol. Membership in certain racial and ethnic groups, including Hispanic, Black, Native American, Asian American, and Pacific Islander populations, is also associated with elevated risk for Type 2 diabetes in children.
The specific tests to request include a fasting blood glucose test, which measures blood sugar after at least eight hours without food. A hemoglobin A1C test, which reflects average blood sugar over the previous three months, provides a broader picture than a single fasting measurement. An insulin level test alongside the fasting glucose can reveal early insulin resistance even when blood sugar is still within the normal range.
Understanding when and how diabetes in children begins is the first step toward preventing or delaying it in your family. The time to act is not after a diagnosis. It is now, regardless of your child’s current health status, because the habits established in these early years will shape their metabolic health for the rest of their lives.
Looking for comprehensive guidance on caring for your baby? Our book ‘How to Care for Children: From Birth to Age 2’ combines professional childcare expertise with evidence based child development research. Written by Kelly and Peter, this guide provides clear, reliable advice rooted in real world childcare. Available in English, Spanish, and Portuguese on Amazon.
Click the link below your preferred language to get your copy!


1. Can a child get diabetes from eating too much sugar?
The relationship between sugar consumption and diabetes in children depends on the type of diabetes. Type 1 diabetes is an autoimmune condition with no known dietary cause, meaning it cannot be caused by sugar consumption. Type 2 diabetes, however, has a strong dietary and lifestyle component. Excessive consumption of added sugars, particularly high-fructose corn syrup, sugary beverages, and ultra-processed foods, contributes to insulin resistance over time, which is the primary pathway to Type 2 diabetes. The risk is not from a single sugar-filled meal but from the chronic, daily pattern of high-sugar consumption that is normalized in many modern households.
2. What is the difference between Type 1 and Type 2 diabetes in children?
Type 1 diabetes is an autoimmune condition in which the immune system destroys the insulin-producing cells of the pancreas. It cannot currently be prevented and requires daily insulin administration for the child’s survival. Type 2 diabetes develops when the body becomes resistant to insulin over time, typically driven by diet, physical inactivity, and genetic predisposition. Type 2 diabetes in kids is growing rapidly and, in many cases, can be prevented or significantly delayed through family lifestyle changes. The two conditions require completely different medical management and carry different long-term implications for the child and family.
3. What are the first signs of diabetes in children that parents should watch for?
The most frequently missed early diabetes symptoms in children include excessive thirst that cannot be satisfied, unusually frequent urination including nighttime bedwetting in a previously dry child, unexplained weight loss despite normal appetite, persistent fatigue, and blurred vision. Dark, velvety skin patches in body folds, known as acanthosis nigricans, are a visible sign of insulin resistance that often appears before any formal diabetes diagnosis. If your child shows two or more of these signs simultaneously, a blood sugar evaluation with your pediatrician is warranted without delay.
4. Are hidden sugars in children’s food really that dangerous?
Yes, and the research is consistent on this point. Hidden sugars in children’s food, particularly high-fructose corn syrup, fruit juice concentrate, agave, and various sugar syrups, are present in dozens of products marketed specifically to families as healthy options. These sugars contribute to insulin resistance, obesity, fatty liver disease, cardiovascular risk, and elevated diabetes risk without the child or parent necessarily consuming anything that appears to be sugary. A single serving of flavored yogurt can contain more added sugar than a small chocolate bar, and it is marketed as a nutritious snack.
5. At what age can children develop Type 2 diabetes?
Type 2 diabetes can develop at any age, including in preschool-aged children, though it is most commonly diagnosed during puberty when hormonal changes naturally create a period of reduced insulin sensitivity. The average age of Type 2 diabetes diagnosis in children in the United States is between 13 and 14 years. However, the metabolic preconditions for this diagnosis, including insulin resistance and prediabetes, can be established years earlier through dietary and lifestyle patterns that begin in the first years of life.
6. Can childhood diabetes be cured?
Type 1 diabetes currently has no cure and requires lifelong management. Type 2 diabetes in children and adults can sometimes be put into remission through significant and sustained lifestyle changes, including substantial improvements in diet quality, regular physical activity, and weight normalization. Remission is not a cure; it means that blood sugar returns to normal ranges without medication. Sustained remission requires maintaining the lifestyle changes indefinitely, and relapse is possible if those changes are not maintained. Early intervention, before the condition has progressed for many years, produces the best remission outcomes.
7. Is fruit juice safe for children with a family history of diabetes?
Fruit juice is one of the most misunderstood components of children’s diets in the context of diabetes risk. Even 100% fruit juice, with no added sugars, delivers concentrated fructose without the fiber that slows absorption in whole fruit. For children with a family history of Type 2 diabetes or signs of insulin resistance, fruit juice should be minimized or eliminated entirely and replaced with whole fruit. Water and plain milk are the recommended default beverages for all children, and particularly for those with elevated metabolic risk.
8. How can I reduce my child’s sugar intake without a major family conflict?
The most effective approach is gradual substitution rather than sudden elimination. Replace one high-sugar product per week with a lower-sugar alternative, starting with beverages since they deliver the most sugar with the least satiety. Introduce water as the default beverage early, before children develop strong preferences for sweetness. When purchasing packaged foods, consistently choose options with the lowest added sugar content within the same category. Involve older children in reading food labels as a family activity, framing it as detective work rather than restriction. Over months, as the household food environment shifts, children’s taste preferences naturally recalibrate toward less sweetness.
9. What long-term health problems does diabetes in children cause?
The long-term complications of uncontrolled diabetes in children are among the most serious in medicine. They include diabetic retinopathy, which can progress to complete blindness; diabetic nephropathy, which leads to kidney failure requiring dialysis or transplant; cardiovascular disease including heart attack and stroke occurring decades earlier than in non-diabetic peers; peripheral neuropathy that can lead to limb amputation; non-alcoholic fatty liver disease; and emerging evidence of connections to cognitive decline and neurodegenerative conditions. All of these complications are directly driven by chronically elevated blood sugar and are substantially preventable or delayed with effective blood sugar management beginning at diagnosis.
10. How do I talk to my pediatrician about screening my child for diabetes?
Requesting diabetes screening is appropriate if your child has two or more risk factors including family history of Type 2 diabetes, overweight or obesity, physical inactivity, signs of insulin resistance such as dark skin patches, high blood pressure, or high cholesterol. Ask specifically for a fasting blood glucose test and a hemoglobin A1C test. If your child is 10 or older and has risk factors, the CDC recommends screening beginning at that age with repeat testing every three years. If you are concerned about insulin resistance specifically, ask whether an insulin level can be measured alongside the fasting glucose, as this can reveal early resistance before blood sugar itself becomes abnormal.